
A recent study by the Centers for Disease Control and Prevention (CDC) found that more than one third of American women are deficient in iodine, and that for these women, exposure to the rocket fuel contaminant perchlorate in food or water can cause a significant and dose dependent decline in thyroid hormone levels. Low thyroid levels, or subclinical hypothyroidism, is an established risk factor in fetal development and can cause IQ deficits, developmental delays, and in severe cases, cretinism.
An Environmental Working Group analysis of the CDC data found that for more than 2 million iodine deficient women nationwide, exposure to perchlorate in drinking water and the food supply, at levels equal to or lower than proposed national and state standards, could lower thyroid hormone levels to the extent that they would require medical treatment to avoid developmental damage to their babies.
Sources: [1, 12]
California's proposed limit for the chemical, perchlorate, could depress thyroid hormone levels in more than 272,000 California women of childbearing age to the extent that they would require medical treatment to protect their babies from IQ deficits and abnormal development. New Jersey's proposed limit could cause such deficiency in 65,000 women in that state.
If applied nationwide, the California proposal would trigger thyroid deficiency requiring treatment during pregnancy in more than 2.2 million women of childbearing age. But the federal government's waste-site cleanup standard for the chemical is more than four times weaker than the California drinking water proposal, extending the risk to millions of additional women and their babies.
EWG's findings show clearly that the perchlorate cleanup standard adopted by the U.S. Environmental Protection Agency, and the safety standards for perchlorate in drinking water under consideration in California and New Jersey, are inadequate to protect the 22 million American women of childbearing age who don't get enough iodine in their diet. Even the stricter drinking water standard already adopted by Massachusetts would cause a decline in women's thyroid levels.
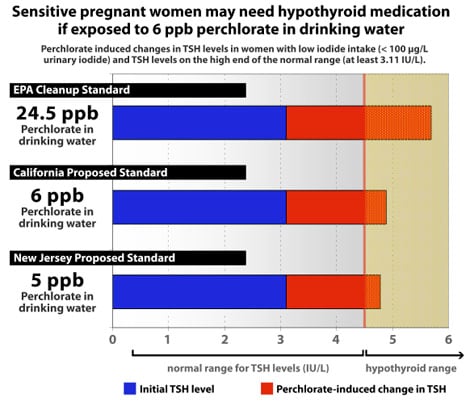
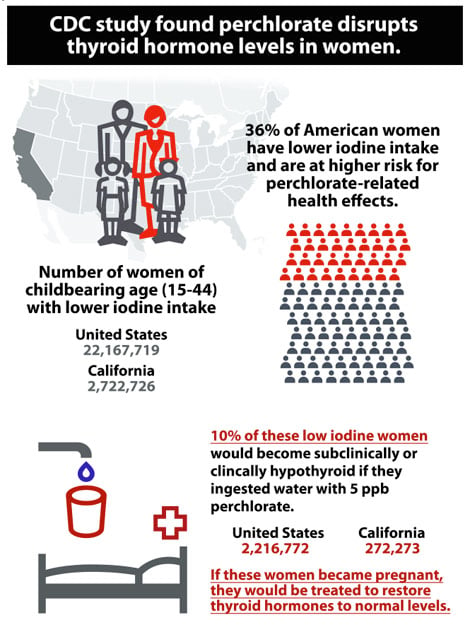
In September 2006, a startling study from the U.S. Centers for Disease Control (CDC) found that in the 36 percent of U.S. women with low iodine intake, almost any amount of perchlorate exposure was linked to a significant change in levels of thyroid hormones. [1] For about 1 in 10 of these women, if they were exposed to 5 parts per billion of perchlorate in drinking water, the resulting hormone disruption would require treatment for sub-clinical hypothyroidism, according to a consensus of clinical endrocinologists. [2]
Perchlorate, the explosive ingredient in solid rocket fuel, has leaked from military bases and defense and aerospace contractors' plants in at least 22 states, contaminating drinking water for millions of Americans. The chemical has also been found widely in supermarket milk, produce and many other foods and plants; in a separate study, the CDC found it in the urine of every person tested. [3 &em; 12] As small changes in thyroid hormone levels during pregnancy &em; even within the normal range &em; are associated with decreased intellectual and learning capacity in childhood, the extensive reach of perchlorate contamination has huge implications for public health. [13, 14]
The CDC's studies are the first major epidemiological research into the potential health impacts of chronic perchlorate exposure. Researchers found a statistically significant, dose-dependent association between perchlorate exposure and changes in thyroid hormone levels in all women in the study.
The effects on thyroid hormones were particularly pronounced in women with lower iodine intake. Among these women, a urinary perchlorate level of only 5 parts per billion was associated with a 16 percent change in thyroid hormone levels, compared to the median level found in the study. The authors noted that 36 percent of U.S. women have iodine intakes in the range identified as "lower" in the study.
The findings were consistent with how we understand hormones to be regulated in the human body, and how we understand perchlorate to exert its toxic effects. [1] But most important are its implications for the drinking water standards and cleanup standards proposed or adopted by several states and the U.S. Environmental Protection Agency.
Under pressure from the Pentagon and the defense industry, EPA has delayed setting a drinking water standard for perchlorate. But in January, after a controversial National Academy of Sciences study &em; since strongly criticized by a federal advisory panel on children's health &em; the EPA adopted a standard for cleanup of perchlorate-contaminated waste sites of 24.5 parts per billion. [15, 16]
California is in the final stages of adopting a perchlorate drinking water standard of 6 ppb, recommended by state scientists before release of the CDC study. The proposed standard in New Jersey is 5 ppb. In July, Massachusetts adopted 2 ppb as the nation's first legally enforceable drinking water standard.
The CDC data show that perchlorate exposure at just 5 ppb will cause significant disruptions in thyroid hormone levels for women who have lower iodine intake. This will translate into significant risks to unborn babies, infants and children, with a very real potential for significant developmental delays and learning deficits in the exposed population.
Applying the results of the CDC study to the California population, EWG estimates that at exposure to 5 ppb of perchlorate in drinking water, 1 in 10 California women of childbearing age with low iodine intake would be diagnosed as sub-clinically hypothyroid. This equals about 272,000 women in California whose exposure to perchlorate in tap water could necessitate treatment during pregnancy for subclinical hypothyroidism, a condition known to increase the risks of long term neurological damage and developmental delays. [2, 17]
It is reckless to adopt a drinking water standard for perchlorate that is such a risk to women and their unborn babies that mothers would need prescription medicine to counteract the threat. And the CDC didn't even look at the impact of perchlorate exposure on infants, children and other adults already suffering from thyroid deficiency.
Broad Implications for CDC Study
To investigate the potential health implications of perchlorate exposure in the general populations, CDC tested urine samples of 2,299 men and women from around the country for perchlorate and compared these findings with the levels of thyroid hormones found in the blood of these same people. The researchers were careful to adjust for factors such as age, race, pregnancy status, and medication use known to affect thyroid hormone levels.
CDC's analysis focused on the association between perchlorate exposure and two kinds of thyroid hormones: T4 and TSH. T4 is the hormone that plays an important role in brain and organ development in fetuses, infants and children and regulates metabolism in adults. TSH (thyroid stimulating hormone) is the hormone that the body makes to stimulate the production of T4. Doctors diagnose hypothyroidism by looking at TSH levels because the level of this hormone is a more sensitive indicator of a person's thyroid status. If TSH is elevated, but T4 levels are still relatively normal, the patient will be diagnosed with mild (or subclinical) hypothyroidism. If the TSH levels are elevated and the T4 levels have dropped below a certain threshold, the patient will be diagnosed with clinical hypothyroidism. [19]
While analyzing the study data, the CDC's researchers discovered that there was a statistically significant relationship between urinary perchlorate and thyroid hormone levels in the 1,111 women tested. But the effects were particularly pronounced in women with lower iodine intake. †1 For women with higher iodine intake, perchlorate exposure was associated with increased TSH. For women with lower iodine intake, perchlorate exposure was associated with both increased TSH and decreased T4 levels. Since 36 percent of American women have iodine intake in the "lower" range as defined by the CDC, this means that more than one-third of all women are at heightened risk for perchlorate-related health effects.
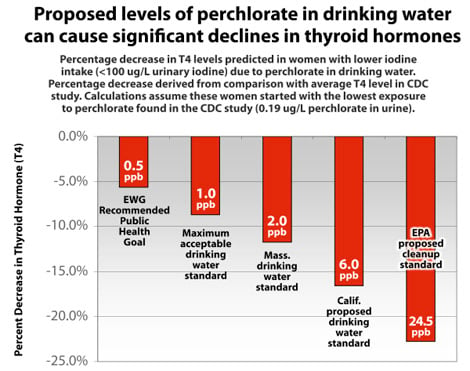
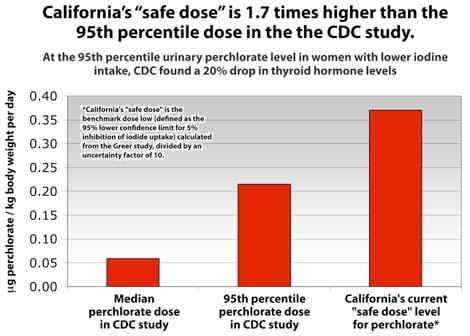
Even more important are the extremely low levels of perchlorate that were associated with thyroid hormone disruptions &em; and the magnitude of these disruptions. The CDC researchers found that if a low iodine woman started with perchlorate exposure corresponding to 0.19 ppb in urine (the minimum level found), and then ingested enough perchlorate through food and/or drinking water to raise her urinary perchlorate level to 2.9 ppb (the median level found), her T4 levels would drop by 13 percent.†2 Similarly, if her urinary perchlorate level increased to 5.2 ppb (the 75th percentile exposure), her T4 levels would drop by 16 percent. The maximum level of perchlorate exposure found was 100 ppb, which translated into a 29 percent decline in T4.
It is reasonable to expect that if a person drank water with 6 ppb of perchlorate, the concentration of perchlorate in their urine would increase by roughly this amount. This is because perchlorate passes through the body unmetabolized in a relatively short time period, and because people pee out about as much water as they drink in a given day. Extrapolating from the CDC's results, therefore, it is clear that all of the current proposed and adopted perchlorate standards will cause significant declines in T4 among women with lower iodine intake.
Sources: [1, 12]
When one also considers the CDC's results for perchlorate-related changes in TSH, the picture becomes even more troubling. As noted above, doctors rely on TSH levels to diagnose mild hypothyroidism. The CDC study found that 10 percent of low iodide women — those that started with TSH levels that were on the high-end of the normal range — were particularly sensitive to perchlorate. For these women, a given change in urinary perchlorate levels was associated with a much higher spike in TSH levels than women who had TSH levels closer to the median. And at a 5 ppb exposure level, these women's TSH values crossed the threshold into the range of subclinical hypothyroidism.
This is notable because the unique physiology of pregnancy and interactions between the mother and fetus makes both especially susceptible to the harmful effects of perchlorate. Maternal T4 is the only source of thyroid hormone for the fetus in the first trimester. Recent studies have shown that the cognitive development of the fetus is impaired in mothers with even mild disruptions in thyroid hormone levels, prompting the medical community to recommend thyroid hormone replacement therapy for pregnant women who are found to have sub-clinical hypothyroidism (mildly elevated TSH but normal T4). [2, 13, 14, 17]
Sources: [1, 2, 12, 17]
Although it might seem that this sensitive group &em; women with low iodine intake with high-normal TSH levels &em; would be a tiny fraction of the population, it actually comprises about 3.6 percent of adult females. This translates into more than 2.2 million U.S. women of childbearing age who, if they drank water contaminated with 5 ppb perchlorate, would have to be medically treated to restore thyroid hormones to normal levels if they became pregnant. At the state level, this translates to more than 270,000 women in California and 65,000 women in New Jersey whose pregnancies would be at risk from perchlorate in drinking water at their state's proposed drinking water levels. Even Massachusetts's 2 ppb standard, adopted earlier this year, can't be considered safe since it would also push some borderline hypothyroid women into the range of mild hypothyroidism.
Sources: [1, 2, 12, 17]
Footnotes
†1 - Defined as <100 µg/L iodine in urine.
†2 - The drop in T4 predicted to be 1.06 µg/dL. The percentage decrease calculated as compared to the average T4 level found in the CDC study (8.27 µg/dL).
Kids Likely at Greater Risk
Infants and children likely more susceptible than adults
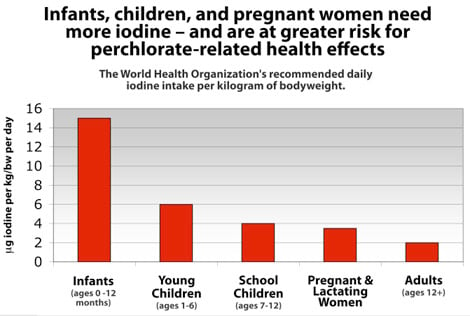
Although the CDC study looked only at individuals ages 12 and over, both new and established research indicates that infants and children may be at even greater risk than the fetus from perchlorate-induced health effects. Perchlorate interferes with the thyroid's ability to take up iodine, a necessary building block for thyroid hormones. For this reason, individuals with higher iodine requirements will likely be more susceptible to adverse health effects than those who need less iodine. And it has long been known that infants and children have higher iodide requirements than adults or even pregnant women.
Sources: [20]
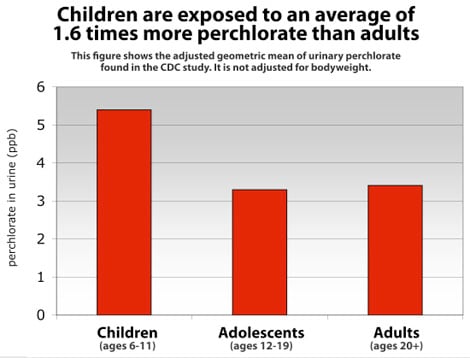
The World Health Organization (WHO) recommends that young children and infants and ingest 3 and 7.5 times more iodine per kilogram of body weight than non-pregnant adults, respectively. For pregnant and lactating women, WHO recommends that they ingest about 1.5 times as much iodine than other adults. [20] These higher iodine requirements alone suggest that infants and children may be even more likely to suffer from perchlorate-related changes in thyroid hormone levels in adults. But even more troubling is new research suggesting that children also have elevated perchlorate exposures as compared to adults.
In a second CDC study published this month, researchers tested more than 2800 urine samples for perchlorate and found that children ages six to eleven had an average of 1.6 times more perchlorate in their urine than adults. [12] Given the large sample size and the fact that the study population was chosen to be nationally representative, these findings should be considered statistically reliable. And although the study did not look at children under six, it raises concerns that infants and younger children may also be exposed to elevated levels of perchlorate. This is especially true since infants and young children have much higher intakes of drinking water in proportion to their body weight &em; and the fact that perchlorate has been detected in human breast milk at moderate to high levels. [10, 21]
Sources: [12]
Much attention has rightly been given to the disruptions of normal thyroid hormone levels during pregnancy and the subsequent effects on IQ. These studies clearly indicate that the fetus is a population of concern when it comes to perchlorate exposure. But it is also important to note that recent research shows that infants can suffer permanent neurological deficits from short-term thyroid hormone insufficiency. [21] When such findings are considered together with infants' and children's higher iodide requirements and perchlorate exposures, it is clear that regulators must include a large uncertainty factor to account for children's increased vulnerability when basing a drinking water standard on a study that only looked at effects on adults.
Of course, pregnant women and children are not the only vulnerable population who must be protected. As noted earlier, the CDC study found that women with lower iodine intake were more sensitive to perchlorate than women with normal levels. The study also found that women with low iodide intake who also were on the high end of the normal range for a thyroid hormone known as TSH were more sensitive to perchlorate than women with TSH levels closer to the median. In addition, people who are already hypothyroid, people who smoke (smoking can interfere with the thyroid's ability to use iodine), and/or who are elderly and therefore more prone to thyroid problems may also be extra sensitive to perchlorate and must be protected.
This point has been underscored by the National Academy of Sciences, which noted that in a 2005 report that "pregnant women, infants, and children, and people who have low iodide intake or pre-existing thyroid dysfunction, the dose [of perchlorate] required to cause a decrease in thyroid hormone production may be lower [than for non-pregnant adults]." [22]
Proposed Standards Based Upon Inadequate Study
The six parts per billion (ppb) drinking water standard for perchlorate proposed by the state of California is based on the findings of a short-term study with a very small sample size, now known to be wholly inadequate to detect perchlorate-related health effects. The same is true for the drinking water standards proposed in New Jersey, the clean-up standard adopted by the US EPA, and to a lesser degree the drinking water standard recently adopted by Massachusetts.
This study supporting the California proposed standard, known as the "Greer study," dosed 37 healthy adults with perchlorate for just 14 days. [23] The study did not include any measurement of iodide status, which the CDC study has subsequently shown to be a key variable. And when US EPA analyzed the study design, the agency found that it did not have sufficient statistical power to detect effects at low doses due to the small number of individuals in each dose group. (The lowest dose group included only seven individuals &em; six females and one male.) [24, 25]
The authors averaged data within dose groups to claim that the lowest dose of perchlorate caused no effects on iodide uptake by the thyroid. Closer examination of the data, however, shows that four of the seven individuals did have perchlorate-related reductions in iodide uptake. [16] With the CDC study in hand, we now know that these effects occur in the population, particularly in iodine deficient women, and that the proposed California standard would not protect the public health.
Sources: [1, 12, 27]
Increased iodine supplementation not a solution
After the CDC study was published, some observers suggested that it would be cheaper and easier to increase iodine intake in the general population to alleviate perchlorate-related health issues than to clean up contaminated drinking water supplies. Although EWG supports consideration of iodization of salt and other foods as a partial preventive measure for hypothyroid conditions in the population, it is not an effective solution to the problem of perchlorate contamination of drinking water and should not be used as a justification to allow what would otherwise be unacceptably high levels of perchlorate exposure, as would occur under the current proposal for a standard of 6 ppb perchlorate in tap water.
First, iodine supplementation is difficult to control in terms of how much iodine an individual gets. Iodine fortification of food was actually reduced in the US, for example, in the 1980's because of concerns that excess iodine intake could cause autoimmune thyroid disease and thyroid cancer. [26, 28] Increased iodization of salt would also be limited in effectiveness because some individuals must limit their salt intake due to high blood pressure, kidney disease, or other health issues, and because infants do not eat solid food to which iodized salt could be added.
It is also important to point out that even with modern public health practices, some degree of nutrient deficits are essentially impossible to avoid in the general population. The extra sensitivities of these individuals must be considered &em; especially when this population extends to more than one-third of all women. Finally, it is simply not ethical to ask the population to increase their iodized salt intake simply to counteract the effects of a chemical contaminant in their bodies.
Conclusion
While California and other states should be commended for moving forward to set standards for perchlorate in drinking water given the federal government's failure to do so, it would be unwise to finalize these standards until the results of the CDC study are amply taken into consideration. With the CDC study showing that even less than 1 ppb perchlorate in water may pose health risks to women, fully protective drinking water standards must be set as low as possible &em; at no more than 1 ppb &em; and revised downward as detection and cleanup technology improves.
About This Report
Principal authors: Renee Sharp and Anila Jacob, MD, MPH
Editors: Bill Walker and Richard Wiles
Web design and graphics: T.C. Greenleaf
This report was made possible by the support of The California Wellness Foundation and other funders. Opinions expressed in this report are those of the authors and editors, who are responsible for any errors.

